Toward Evidence-Based Practice: Use of Scientific Literature Reviews with a Focus on Suicide Risk and Abortion
![]()
A.I.R.V.S.C.
Association for Interdisciplinary Research in Values and Social Change
by
Priscilla K. Coleman, Ph.D.
Human Development and Family Studies
Bowling Green State University
Volume 23, Number 1 -- Spring 2011
Reproduced with Permission
Research Bulletin
Informed consent for medical procedures occurs when patients adequately understand their condition along with the benefits, risks, and limitations of treatment alternatives.[1] Health care professionals are responsible for educating patients in a manner that reflects the current scientific literature; however, recent concern raised in the medical community suggests this is a too infrequently realized ideal.[2] Clinicians often lack the requisite skills and time to interpret the ever-expanding scientific literature necessary to optimally inform their practice and provide patients with accurate up-to-date synopses of the literature that facilitate truly informed health care choices.[2] In a report released by the U.S. Institute of Medicine titled "Crossing the Quality Chasm" the authors noted "Medical science and technology have advanced at an unprecedented rate during the past half-century. In tandem has come growing complexity of health care, which today is characterized by more to know, more to do, more to manage, more to watch, and more people involved than ever before."[2] Research which should be driving positive changes in medical practice is often ignored for many years, sometimes decades.[2] As described in the Institute of Medicine publication referred to above: "It now takes an average of 17 years for new knowledge generated by randomized controlled trials to be incorporated into practice, and even then application is highly uneven."
Sackett and colleagues defined evidence-based medicine as a process integrating individual clinical expertise with the best external evidence and patient choice to maximize the quality and quantity of life for the individual patient.[3] Ironically as awareness of the need for evidence-based medicine has grown over the last decade in the U.S. and strategies are being developed to revamp health care delivery to close the gap between knowledge and practice, the divide is greater than ever relative to conferring accurate unbiased information on risks of abortion to women considering the procedure. Political, ideological, and social forces undoubtedly compete with efforts to conduct, publish, and disseminate straightforward appraisals of a rapidly accumulating world literature on the health consequences of abortion. The goal of this report is not to analyze the complex context for what appears to be a significant evidence-based practice lag in this domain of reproductive health, but to initiate candid discussion of the schism and describe a concrete strategy for deriving valid reviews of the literature. A dispassionate examination of the discrepancies between what is known and what is shared with women seeking abortions should ultimately foster accuracy in pre-abortion counseling and encourage true informed consent, thereby enhancing the quality of health care delivery.
Empirical data and informed consent practice: The example of risk for suicide
Have abortion providers been offering accurate information to the millions of U.S. women considering abortion each year and the more than 1.2 million[4] who ultimately make the choice to terminate a pregnancy?
The answer to this question requires the following:
- 1) a thorough unbiased evaluation of the scientific literature;
- 2) an analysis of informed consent materials used by abortion providers; and
- 3) an analysis of the degree of congruence between what is known and what is shared with women.
To gain a handle on the world literature pertaining to abortion problems, peer-reviewed studies published in reputable journals must be evaluated systematically using established scientific protocol. Moreover, due to the highly politicized nature of abortion and related concerns of bias pertaining to reviews conducted by individual scientists and professional organizations, ideally evaluation teams will be comprised of people who hold a variety of views regarding the morality and legality of abortion. In the section that follows, a strategy for evaluating the best scientific evidence pertaining to the psychological effects of abortion is offered. For simplicity, this illustrative discussion will be restricted to only one of many well- researched mental health outcomes of abortion, suicidal behavior.
Systematic analysis of the literature to assess risk and causality
A risk factor is any variable that has been established to increase the likelihood of an individual experiencing an adverse outcome. Risk factor data is used in medicine and psychology to understand etiology, warn patients of potential problems associated with various exposures, and develop effective prevention and intervention protocols to maximize health. In the absence of the ability to introduce strict experimental control, risk factors for negative outcomes are established over time through the two primary scientific steps described below.
1. Analysis of each individual study.
Each study published in a peer-reviewed journal is examined to assess the quality of evidence suggestive of a causal link between abortion and negative outcomes.[5,6] Three criteria are employed for this purpose:
a. Abortion must be shown to precede the mental health problem (time precedence). This is accomplished with prospective or longitudinal data collection.
b. Differences in abortion history (abortion, no abortion) must be systematically associated with differences in mental health status (covariation).
c. All plausible alternative explanations for associations between abortion and mental health must be ruled out using one or more of the methods described below.
- i. Measure and statistically control for known predictors of abortion.
- ii. Match groups on all variables known to be related to abortion.
- iii. Measure potential confounding variables and introduce them as additional variables to assess their independent effects.
- iv. Sample from homogeneous populations to eliminate potential confounds.
2. Integrative analysis.
After evaluating individual studies for causal evidence linking abortion to mental health, scientists assess the consistency and magnitude of associations across all available studies.
a. Consistency refers to repeated observation of an association between abortion and mental health revealed in several studies using different people, places, and circumstances.
b. Magnitude (or strength of effect) refers to whether the associations between abortion and mental health problems are slight, moderate, or strong. Strong associations across various studies are more likely causal than slight or modest associations.
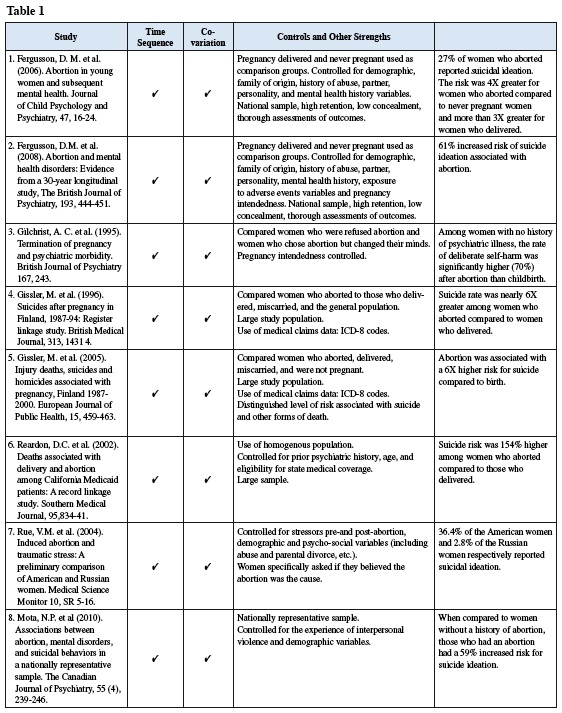
As indicated in Table 1, when these criteria are applied to all peer-reviewed reports of abortion and increased risk for suicide published in English in psychology and medical journals from 1994 through 2009, there is evidence for abortion operating as a significant risk factor for suicide ideation and suicide.[7-13] Specifically, the available studies are large scale, prospective in nature, and they incorporate a variety of different types of comparison groups as well as additional control techniques, all of which significantly enhance the validity of the findings. On a side note, there are also numerous studies affirming associations between abortion and both depression and substance abuse[14-20], which are primary risk factors in the etiology of suicidal behavior.[21] Therefore, available data indicate that abortion is directly and indirectly associated with suicidal ideation and suicide.
Incorporating Attributable Risk and Population Attributable Risk statistics
In addition to the need for literature reviews that adhere to a standardized and accepted methodology, more focused attention should be given to the design of individual studies to generate results that are readily translatable into useful, easily comprehended information for professionals counseling women seeking abortion services. Since randomized trials are not permissible with abortion, new studies ideally meet the conditions for establishing causality as outlined above.
Future individual investigations should also be geared toward incorporating under-used data analysis techniques such as the Attributable Risk (AR) and Population Attributable Risk (PAR) statistic. These statistics are identified as measures of impact as they incorporate data on the frequency of a particular disorder (incidence or prevalence) and a measure of the degree of association between an exposure (e.g., abortion) and an outcome (e.g., suicidal behavior). In a review of epidemiological studies published between 1966 and 1996 employing attributable risk, Uter and Pfahlberg[22] identified only 334 reports across all medical specialties. The sample included studies incorporating many different types of exposures (alcohol, drug use, infections, environmental factors, nutritional factors, psychosocial factors, etc.) for widely varying diseases including cancers, cardiovascular diseases, and psychiatric disturbances. However, this literature was devoid of studies examining the impact of induced abortion on any health outcomes.
AR is the proportion of the incidence of a disorder (e.g., suicidal behavior) in the exposed group (e.g. women who have aborted) that is directly due to the exposure (the abortion procedure).[23] In other words, AR reflects the incidence of suicidal behavior in women who abort that would be eliminated if the abortion had not occurred. The AR is sometimes referred to as excess risk and it is calculated rather simply by subtracting the incidence in the unexposed (women who have not aborted) from the incidence in the exposed (those who have aborted). Attributable risk percent (AR%) reflects the incidence of a disease in the exposed that is due to the exposure. In our example it reflects the proportion of suicidal behavior that would be eliminated if the abortions had not occurred. The AR% is derived by dividing the AR by the incidence in the exposed and then multiplying this product by 100. In situations wherein the absolute frequency of a disorder is not known, these formulas are modified slightly with a relative risk or odds ratio incorporated.
PAR provides an estimate of the public health impact of a particular exposure as it is the portion of the incidence of a disease in the entire population (not just the exposed) that is directly due to the exposure or that would be eliminated if the exposure did not occur. The PAR is calculated by subtracting the incidence in the unexposed (e.g. rate of suicidal behavior in women who have not aborted) from the incidence in the total population (e.g. rate of suicidal behavior in those with and without an abortion history). To derive the PAR%, the PAR is divided by the incidence in the total population and multiplied by 100. When population exposure rates are not available, estimation is achieved as indicated for the AR with the basic formulas modified using the relative risk or odds ratio statistic.
Ideally future studies employing the AR and PAR will include assessments of numerous potentially confounding third variables with statistically adjusted measures of association employed to derive accurate estimates of the unique impact of abortion. In the comprehensive review of attributable risk studies cited above, the authors reported that only 37.5% actually included statistical adjustment.[22]
The PAR is most useful and appropriate when the association between an exposure and an outcome are believed to be causal and for many years there has been debate about whether or not abortion causes mental health problems. The extensive world literature now supports a causal role for a significant portion of women seeking abortions .[7-11],[13-20],[24],[31],[32]
Future investigative efforts designed to examine the PAR relative to induced abortion and various mental health outcomes should also include calculation of the PAR for other widely accepted predictors of mental health problems such as histories of abuse, exposure to other significant stressors of various forms, a family history of mental illness, etc. in order to assess the magnitude of the PAR for abortion in the etiology of psychological disorders in comparison to other well known causes. This information could prove quite valuable as professionals offer a broader context for women engaged in abortion decision-making.
To summarize, both the AR which indicates the difference in rate of suicidal behavior among women with and without an abortion history (excess risk) and the PAR which describes how much of the overall incidence of suicide in the population (women with and without an abortion history) is directly due to abortion are easy to calculate and offer tangible information that can be readily conveyed to health care professionals and women considering an abortion. An example to illustrate the utility of the public health information derived from calculation of the PAR is provided below.
In an article published in 200924 the PAR was calculated for abortion as a cause of Major Depression among many other disorders. In this study, PARs for several anxiety, mood, and substance abuse disorders were found to range from 4.3% to 16.6%. The PAR for Major Depression based on abortion was equal to 4.3%. According to the U.S. Census Bureau, there are 62,117,211 women of reproductive age living in the U.S. [http://www. census.gov/popest/national/asrh] and one year prevalence rates for Major Depression in women between the ages of 18 and 54 have been reported by the U.S. Surgeon General to equal 6.5% [http:// www.surgeongeneral.gov/library/ mentalhealth/toc.html]. Based on this rate, 4,037,618 women (6.5% of 62,117,211) experience Major Depression annually in the U.S. The PAR for Major Depression resulting from abortion is equal to 4.3%, meaning 173,617 women of reproductive age (4.3% of 4,037,618) experience Major Depression each year as a direct result of abortion.
Using the PAR for Major depression in conjunction with data from the U.S. Census Bureau and the U.S. Surgeon General's Office, the number of annual suicide deaths directly attributable to abortion can be calculated. Estimates regarding the percentage of individuals who commit suicide in response to Major Depression range from 1% to 15%. Applying the most conservative 1% figure, the number of suicides per year attributed to abortion equals 1736. However, given the differential rates of suicide between males and females, the estimate of the number of suicide deaths should reflect the fact that women are less inclined than men to commit suicide. The gender ratio of men to women committing suicide is 4:1 [http://www.who.int/ mental_health/prevention/suicide_ rates/en/index.html]. If the 1% of cases of major depression resulting in suicide is cut down to .25% to reflect this gender difference, there are no fewer than 434 suicide deaths (.25% of 173,617) each year in the U.S. which are directly attributable to abortion. There are approximately 8109 female suicides annually in the U.S. according to the National Institutes of Mental Health [http://www.nimh.nih.gov/ health/publications/suicide-in-the- us-statistics-and-prevention/index. shtml]. Therefore abortion-related suicides account for over 5%.
Unsubstantiated informed consent practice
The Planned Parenthood organization, which is widely recognized as the largest abortion provider in the U.S. has claimed that abortion is safer than childbirth with the abortion-related death rate cited as 1 in 100,000 or 12 cases per year (www.plannedparenthood. org). On the Planned Parenthood website the following information is provided, "In extremely rare cases, very serious complications may be fatal. The risk of death from childbirth is 11 times greater than the risk of death from an abortion procedure during the first 20 weeks of pregnancy. After 20 weeks, the risk of death from childbirth and abortion are about the same." No peer-reviewed research articles are cited to back this claim. The statement does not specifically address death by suicide and there is no mention of abortion as a risk factor for suicidal behavior anywhere in materials produced by Planned Parenthood. Nevertheless, examination of the empirical evidence above pertaining to abortion-related suicide deaths alone renders this statement quite inaccurate.
Suicide deaths are rarely, if ever, linked back to abortion in state reporting of death rates for the reasons indicated below and suicides are often not recorded on death certificates.[25] The International Classification of Diseases (ICD-9) defines maternal death as one that occurs during pregnancy or within 42 days of the termination of pregnancy. Pregnancy-associated deaths occurring outside this window are not captured in the data. When a death is violent, a recent birth may not be recorded and a recent abortion is even less likely to be mentioned. These issues pertain specifically to suicide; however there are numerous additional reasons why the more general statistics related to the risk for death associated with abortion vs. childbirth are unreliable.[25,26] The National Center for Health Statistics (NCHS) provides maternal mortality information and the Center for Disease Control (CDC) provides abortion mortality statistics. Different standards and methods of data collection are used by the two systems rendering comparisons between the two inappropriate. The abortion data collection system is particularly prone to missing a large percentage of deaths. Specifically, coding rule 12 of the ICD-9 requires deaths due to medical and surgical treatments to be reported under the complication of the procedure (e.g., infection) rather than the treatment (e.g., induced abortion). Further, most women leave abortion clinics within hours of the procedure and go to hospital emergency rooms if there are complications. Finally, abortion reporting is not required by federal law and only 27 states currently report abortion complications. A comprehensive understanding of the connection between abortion and suicide therefore requires attention to the peer-reviewed literature as opposed to relying on the incomplete data gathered by governmental agencies.
Conclusion
In this article an approach to examining the existing abortion and mental health literature in a systematic, unbiased manner was offered using the most serious potential outcome, suicidal behavior to illustrate. The scientific literatures related to abortion and anxiety[13,24,27,28] depression[7,8,17-20,24] and substance abuse[7,8],[14-16],[24] have matured to the point wherein it would be beneficial to conduct a thorough analysis of the evidence pertaining to these other effects using the strategy outline above. Researchers interested in conducting reliable reviews of the literature might also consider a quantitative evaluation involving calculation of attributable risk statistics from previously published studies if results contain both frequency data and relative risk or odds ratios. Moreover, as illustrated above, future studies should incorporate measures of impact (AR and PAR) that are inherently easy to comprehend and provide an excellent basis for informed consent protocols. In addition to the study described above by Coleman and colleagues[24], only one other study published in English has included calculations of attributable risk. New Zealand researchers led by Fergusson published a longitudinal study in which abortion-related PAR percentages were found to equal between 1.5% and 5.5% with a composite index of psychiatric morbidity used as the outcome8.
Innovative approaches that actively rely on long established scientific methods and make use of published data offer considerable hope for bringing more cohesion to a complex literature that for many years was fraught with conflicting results and polarized interpretations. The success of such an effort will ultimately require a commitment on the part of scientists, leaders of academic and professional organizations, and journal editors to set aside their personal ideological commitments, look honestly at all the published data, and work in concert on behalf of the millions of women who consider abortion and have the right to information that will facilitate appropriate decision-making.
Table 1: click for original
References
- 1. Sheridan SL, Harris RP, Woolf SH. Shared decision making about screening and chemoprevention. A suggested approach from the U.S. Prevention Services Task Force. American Journal of Preventive Medicine 2004; 26:56-66.
- 2. Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
- 3. Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn't. British Medical Journal 1996; 312:71-72.
- 4. Guttmacher Institute. Facts on induced abortion in the United States. In Brief, July 2008. http://www.guttmacher.org/ pubs/fb_induced_abortion.html.
- 5. Hill BA. The environment and disease: Association or causation? Proceedings of the Royal Society of Medicine 1965; 58: 295-300.
- 6. Susser M. Judgment and causal inference: Criteria in epidemiologic studies. American Journal of Epidemiology 1977; 105: 1-15.
- 7. Fergusson DM, Horwood J, & Ridder EM. Abortion in young women and subsequent mental health. Journal of Child Psychology and Psychiatry 2006; 47: 16-24.
- 8. Fergusson DM, Horwood JH, & Boden JM. Abortion and mental health disorders: Evidence from a 30-year longitudinal study, The British Journal of Psychiatry 2008; 193, 444-451.
- 9. Gilchrist AC, Hannaford P, Frank P, & Kay C.Termination of pregnancy and psychiatric morbidity. British Journal of Psychiatry 1995; 167: 243.
- 10. Gissler M, Hemminki E, Lönnqvist J. Suicides after pregnancy in Finland, 1987-94: Register linkage study. British Medical Journal 1996; 313: 1431-4.
- 11. Gissler M, Berg C, Bouvier-Colle M-H, Buekens P: Injury deaths, suicides and homicides associated to pregnancy, Finland 1987-2000. European Journal of Public Health 15 (5): 459-463, 2005.
- 12. Reardon DC, Ney P, Scheuren F et al. Deaths associated with delivery and abortion among California Medicaid patients: A record linkage study. Southern Medical Journal 2002; 95: 834-41.
- 13. Rue VM, Coleman PK, Rue JJ, & Reardon, DC. Induced abortion and traumatic stress: A preliminary comparison of American and Russian women. Medical Science Monitor 2004; 10: SR 5-16, 13-20.
- 14. Coleman PK. Induced abortion and increased risk of substance abuse: A Review of the evidence. Current Women's Health Reviews 2005; 1:21-34.
- 15. Coleman PK. Resolution of unwanted pregnancy during adolescence through abortion versus childbirth: Individual and family predictors and consequences. Journal of Youth and Adolescence 2006; 35: 903-911.
- 16. Coleman PK, Reardon DC, Rue V, Cougle J. Prior history of induced abortion in relation to substance use during subsequent pregnancies carried to term. American Journal of Obstetrics and Gynecology 2002; 187: 1673-78.
- 17. Dingle K, Alta R, Clavarino A et al. Pregnancy loss and psychiatric disorders in young women: An Australian birth cohort study. The British Journal of Psychiatry 2008; 193: 455-460.
- 18. Pedersen W. Abortion and depression: A population-based longitudinal study of young women. Scandinavian Journal of Public Health 2008; 36 (4): 424-8.
- 19. Rees DI & Sabia J J. The Relationship Between Abortion and Depression: New Evidence from the Fragile Families and Child Wellbeing Study. Medical Science Monitor 2007; 13(10): 430-436.
- 20. Thorp J, Hartman K, Shadigan E. Long-term physical and psychological health consequences of induced abortion: Review of the evidence. Obstetrics and Gynecology Survey 2003; 58:67-79.
- 21. Gliatto MF, & Rai AK. Evaluation and treatment of patients with suicidal ideation. American Family Physician 1999; 59: 1500-6.
- 22. Uter A, Pfahlberg A. The application of methods to quantify attributable risk in medical practice. Statistical Methods in Medical Research 2001; 10: 231-237.
- 23. Cole P. McMahon B. Attributable risk percentage in case control studies. Brit. J. Prev. Soc. Med 1971; 25: 242- 244.
- 24. Coleman PK, Coyle CT, Shuping M, & Rue V. Induced Abortion and Anxiety, Mood, and Substance Abuse Disorders: Isolating the Effects of Abortion in the National Comorbidity Survey. Journal of Psychiatric Research 2009; 43: 770-776.
- 25. Reardon DC, Strahan TW, Thorp JM & Shuping MW. Deaths associated with abortion compared to childbirth: A review of new and old data and the medical and legal implications. The Journal of Contemporary Health Law and Policy 2004; 20: 279-327.
- 26. Saul R. Abortion reporting in the United States. Family Planning Perspectives 1998; 30: 244-247.
- 27. Bradshaw Z, Slade P. The effects of induced abortion on emotional experiences and relationships: A critical review of the literature. Clinical Psychology Review 2003; 23; 929-958.
- 28. Cougle J, Reardon DC, Coleman PK, Rue VM. Generalized anxiety associated with unintended pregnancy: A cohort study of the 1995 National Survey of Family Growth. Journal of Anxiety Disorders 2005;19: 137-142. References
Article copyrights are held solely by author.
[ Japan-Lifeissues.net ] [ OMI Japan/Korea ]